Ambulance rides, deathbeds and the meaning of life
What hospice patients taught me as a first responder
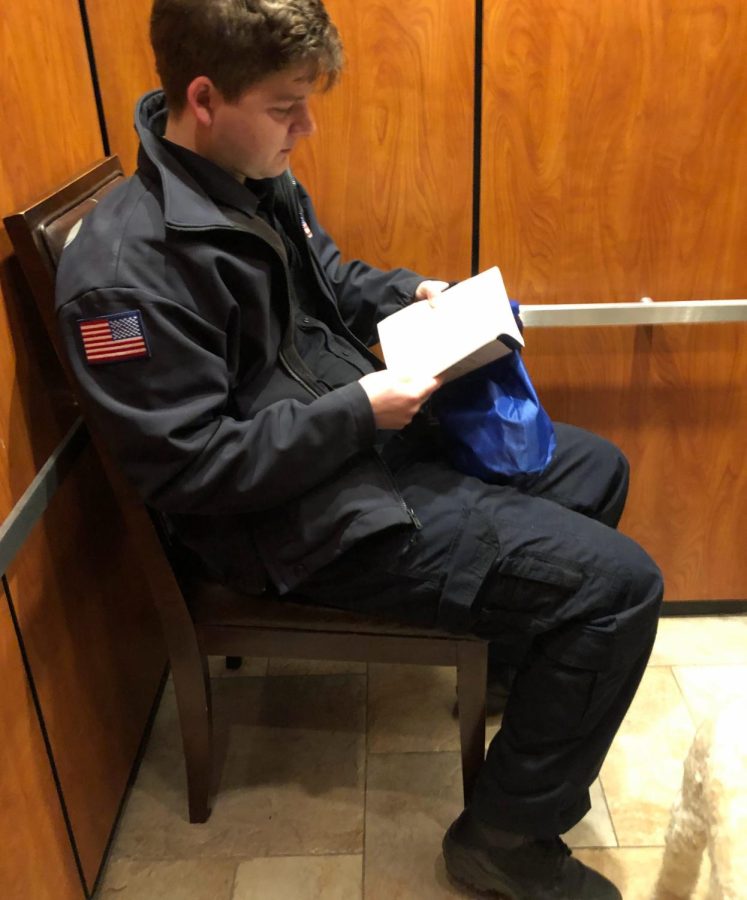
Cole Christensen sits on a chair, reading a book in an elevator at his apartment complex after working a shift for a private ambulance company on Dec. 20, 2021.
For about a year, I worked full-time as an Emergency Medical Technician (EMT). While EMT’s are better known for 911 emergencies, driving lights and sirens in our ambulances, we also transport non-emergent patients who have an altered mental status or are unable to maintain a sitting position. Hospice patients commonly require ambulance transport, going from the hospital to their residence or a hospice center.
Unlike other patients who hope to improve, those receiving hospice care are being transferred from a stretcher to their deathbed, and our job is to make it as painless as possible. Think of the grim reaper with a side-hustle as an Uber driver.
My first hospice patient was tall, thin as a skeleton, and closer to dying than any of the others. His head was tilted to the left, and he couldn’t speak or comprehend what people were saying. I was training at the time, and the only seat available was on the side-bench, the exact direction he was facing. The man stared expressionlessly while the paramedic training me went into great detail over the pain he was going through and his likelihood of dying right there in the 30-minute ambulance ride.
That call made me very emotional. I remember having some larger takeaway that could’ve filled the whole article, but I completely forgot what it was. It’s not surprising. As you get more patients and have the same repetitive experiences, you become desensitized to it all.
While most hospice patients like the man are confused, some are fully alert and capable of having deep conversations. Those conversations were my favorite part of the job, but it gets to a point where they repeat as much as the experiences.
Shortly before quitting, I transported this tiny old woman. She was trying to give me life advice– something about being happy– but could only speak in a whisper, and I had to lean in to understand her. However, I needed to finish her patient care report and couldn’t do it while leaning in. We were assigned for another call afterwards, and if I chose to listen, I would’ve had to choose later between her report and eating lunch. If I chose to eat lunch, I would’ve had to stay late and finish it at the station, so I chose to do the report and pretend like I was listening.
To add to the guilt, she apologized for annoying me whenever it seemed like I was solely focused on the report. I explained that I had to do it, but I could listen at the same time. She continued talking, and whenever it felt fitting, I nodded and said “okay” or “uh-huh.”
I have received advice from many patients, and it could be summarized in two categories: “live a fulfilling life” and “make new experiences.” I can’t deny that the woman was different, but it would be exhausting to take in everyone’s advice on the off-chance that it’s something you haven’t heard before. Eventually, you lose time and patience, listening to similar lectures over and over again.
It’s no fault of the elderly for their lack of originality; it is still good advice and if I was in their position, what would I say differently? Could you think of something beyond a fancier version of fulfillment or new experiences?
There is a third option that’s not necessarily advice but points at a virtue that diverts from the optimism of those two categories. “Do nothing”– do not desire fulfillment, do not desire new experiences, and don’t desire anything outside of one’s own bubble, a bubble not blown up with desire, but molded with indifference.
I call this group the “non-doers.” They don’t explicitly argue against the positive sentiment of people like the whispering patient, and will likely agree with whatever she said, but when the opportunity to pursue fulfillment or new experiences is provided, they don’t take it.
For example, I transported this one patient who moved to a country town an hour west of Aurora, Illinois for a job he only accepted for the money. According to him, there was nothing to do in the town. When retirement came, he didn’t have any hobbies or ambitions to travel and remained. The patient missed the job he put up with all those years– not because of its enjoyment– but because of the boredom he faced now.
He had the opportunity to meet new people in areas where there is more to do. It could have been a life he personally identified to a greater extent, leading to a more fulfilling one, but we will never know because he never took that chance.
It would be excessive and unfair to place the title of “non-doer” on patients based on a single ambulance ride, but I have had a lot of people display characteristics in that category. A surprising amount, actually.
I transported another hospice patient who, in contrast to the rural patient, moved to Chicago from the suburbs. I said that I lived in the suburbs myself and would also like to move to the city someday. She made a weird face and, in a rude tone, said “Why?” I told her why, for the art, music, bars, and new people. She just shrugged and said she moved for a boyfriend.
It surprised me when she made a face, especially since I wanted what she had. Even so, it’s ignorant to not consider why someone would choose to remain in the suburbs. Chicago is expensive. Rent, food, bars, and live music costs more than the suburbs, which are also less crowded and have better infrastructure. The city attracts doers and creates non-doers simultaneously.
Personally, I can’t wait to move out of the suburbs. However, community college is cheap, I like my current job, and my parents are easy to live with. It’s a feasible life, but that doesn’t change my desire to mix it up and start fresh somewhere else.
In a way, I envy the types of patients who are disinterested in working towards fulfillment or new experiences. Imagine a life where you didn’t put so much energy towards dreams or goals, and you stick with your current job for decades, and marry your high school sweetheart, and get a 30-year mortgage on a house close-by without any thought of leaving. How much worse could that be than if you followed the advice on feeling fulfilled and making new experiences?
I fall somewhere between the whispering woman’s advice (assuming it’s generic) and the Chicago patient’s shrug. I’m content in my bubble, but I do get out from time to time and I do wish to pop it altogether. It’s the middle of the two extremes: the optimistic and pessimistic teachings I learned from these hospice patients.
Whichever way you choose, it’s worth noting that the middle may be worse than living in the extremes. I have a desire for new experiences that never gets fully quenched since it’s difficult to make them due to finances and other reasons. In spite of that, the desire is out of my control, and no matter how comfortable it is in my hometown, it feels wrong to push those impulses down to live a simple life.
I try to picture myself in their position, being a hospice patient on the way to a hospice center. What am I supposed to tell the EMT who transports me? I could share what I believe one should do, the generic response, despite being hypocritical for not living up to the standards of doing everything I want in life. I could also say it doesn’t matter in order to discourage the EMT from pursuing what they want to make life easier.
My advice would be to strive to fall somewhere in between. While I did admit that it’s worse than the two extremes, that’s in the context of attempting to pursue one of them. We need to realize how few of us actually live up to the advice they give. The patients I considered to be the non-doers probably have their own interests and unique relationships that no one else will be able to experience. The patients I considered to be doers could’ve chosen to talk about fulfillment and new experiences out of regret for being in the middle themselves. Even if you hate your life, striving for the middle will at least put you in control of your current well-being rather than hope for that control years in the future. Who knows, maybe that sense of control is all we need to be happy.
Also, thinking back to my first hospice patient, it was scary, but also a reminder of how we impact other people’s lives without realizing it. That man was nearly dead, but still managed to inspire an EMT to think in a different way and write about his situation. It makes me wonder: how many strangers have I unintentionally inspired into thinking of things they never thought before? It could be from my clothes, mannerisms, or showing someone an aspect of what my generation is going through. This man had no clue what was happening and yet opened me up to mortality.
So on the ambulance ride to my deathbed, assuming I’m alert, I plan to tell the EMT to have a decent level of fulfillment and some new experiences. If I’m not alert, I hope to teach the EMT what my first hospice patient taught me.
Your contribution will allow us to send students to the National College Media Conference in San Francisco in March 2026. This will grant them an opportunity to learn about about journalism and receive recognition for their work.

Hey! I'm Cole, it's my second year at ECC, and I'm excited to start working for The Observer! I'm working on getting my Associate's in Arts and a Bachelor's...